by Cynthia M. Bulik, PhD
This is Part 2 of a 4-part blog series on the results of the Anorexia Nervosa Genetics Initiative (ANGI) published in Nature Genetics. In Part 1, we revealed the results of the study, Part 3 presents an interview with Professor Patrick Sullivan on next steps, and Part 4 provides some personal reflections and what our results mean for patients, families, and clinicians today.
Between January 2013 and July 2016, we succeeded in obtaining blood samples and clinical information from 13,363 individuals with anorexia nervosa and 9342 controls (people without eating disorders) in five countries around the world. In this post, the second of four, we explain just how we achieved this ambitious goal.
The ANGI Teams
USA. ANGI was coordinated by UNC Chapel Hill. Dr. Cynthia Bulik was the lead Principal Investigator and Dr. Laura Thornton was the Deputy Director. It was Dr. Thornton’s skill in international consortium leadership that made ANGI a success. Dr. Patrick Sullivan from the Departments of Genetics and Psychiatry was a Co-Investigator. Over the years of the study, we had help from numerous faculty and staff including Hunna Watson, PhD, MBiostats (first author and chief analyst), Zeynep Yilmaz, PhD (analyst), Jessica Baker, PhD, and Melissa Munn-Chernoff, PhD. Many other UNC faculty and staff assisted along the way.

ANGI-US: Chris Hilliard, Laura Thornton, Cynthia Bulik, Lauren Metzger, Jessica Baker
Sweden. ANGI-SE was led by Prof. Mikael Landén as site Principal Investigator and coordinated by Dr. Anders Juréus. The large and dedicated Swedish ANGI team held an end of study celebration to mark achieving their recruitment goals.

ANGI-Sweden Final Meeting and Celebration
Denmark. ANGI-DK was centered in Aarhus, Denmark led by Prof. Preben Bo Mortensen, who was joined by Liselotte Petersen, PhD and Janne Tidselbak-Larsen.

ANGI-Denmark: Preben Bo MOrtensen, Liselotte Petersen, Janne Tidselbak-Larsen
Australia. ANGI-AU was led by Prof. Nick Martin and coordinated by Richard Parker. Prof Tracey Wade at Adelaide University was also involved. The professional eating disorders community “down-under” is united by the Australia and New Zealand Academy for Eating Disorders (ANZAED) who were instrumental in recruiting across both Australia and New Zealand. As interest grew in New Zealand, Prof Martin Kennedy and Dr. Jenny Jordan from the University of Otago helped boost recruitment in Australasia. Clinicians and individuals with lived experience across both countries stood at the ready to speak with media about ANGI and help explain the benefits of participation to others with anorexia nervosa.

ANGI-Australia: Prof Nick Martin, Cynthia Bulik, & June Alexander

Prof Martin Kennedy & Jenny Jordan assist from New Zealand
The Strategy
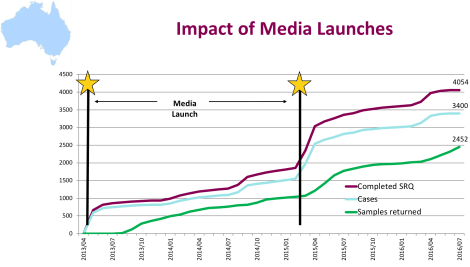
Reaching participants. Knowing that our task was massive, we developed a multi-pronged recruitment strategy that engaged researchers, clinicians, journalists, bloggers, advocacy groups, family members, and individuals with lived experience to assist with spreading the word about ANGI. We developed an outreach strategy that included traditional media, social media, blogs, and other outlets to spread the word about ANGI. The Australian team engaged a PR Firm Viva! Communications who used widespread traditional (TV, radio, print) + digital (online and social) coverage along with national healthcare professional (HCP) and consumer news media. In fact, Viva! Was commended by the Public Relations Institute of Australia National Golden Target Awards for their ANGI campaign. Each time they did a launch, we had a huge bump in in participation, with hundreds of individuals heading to the website to take the survey and enroll in ANGI. Each launch we did (New South Wales, Western Australia, New Zealand) engaged clinicians and people with anorexia nervosa to be available to local and national media outlets around the country ensuring near immediate response and availability of individuals to interview for print, radio, or television.
Denmark was unique. Our work in Denmark differed from the other sites due to their amazing national resource that stores the blood drop from the heel stick at birth. In many countries when a baby is born, they will get a little prick on the heel [phenylketonuria (PKU) test] to check whether a newborn has the enzyme needed to use phenylalanine. Phenylalanine is an amino acid that is needed for normal growth and development. If caught early, a phenylalanine restricted diet can prevent the neurodevelopmental consequences of PKU. Most countries just discard these blood spots after the test is complete, but Denmark wisely stores them under controlled conditions that allows GWAS to be performed on them years and even decades later. In addition, their brilliant health registers allow us to identify everyone in the country who has had a diagnosis of anorexia nervosa at some point in time. We could therefore pull the blood spots from cases identified as having had anorexia nervosa along with controls matched by sex and birth year who have never had the illness. Using this strategy, Denmark contributed samples from 5019 individuals with anorexia nervosa, making them the largest contributor to the ANGI sample.
Lessons Learned
National laws. When doing an international study like ANGI, one learns a lot about international laws. Some countries allowed us to do everything online (consent forms, screening, enrollment), whereas others required telephone contact with research personnel at some point in the process. There is no question that recruitment is smoother when everything can be done online. The best option is perhaps to give participants the option. Some individuals really like the opportunity to tell their story to someone who really cares, whereas others are far more comfortable doing everything digitally.
Making it easy for participants. The technology of genetics advances rapidly. When we started ANGI, it was necessary to get blood from participants, which increased the burden on them to go somewhere to get the blood drawn and sent back for genotyping. This added an additional hurdle, especially in the US where options for phlebotomy are limited. Completion rates accelerated when we hired a mobile phlebotomy company that would come to your home to collect blood for ANGI. In the next iteration of our research, things will be much easier. Thanks to advances in technology, we can now be confident that saliva samples yield high quality DNA. So participation in our ongoing and next studies just require you to spit into a tube and mail it back to us!
Many very ill people are distanced from treatment. One of the early concerns about our social media driven recruitment is that we would attract individuals with anorexia nervosa who were much less ill than the individuals we recruited from treatment centers. This turned out not to be the case, which is very concerning. Many people with severe illness are living with anorexia nervosa in the community without ties to treatment facilities. The reasons for this are presumably many—access, insurance, previous experience with treatment, and an absence of options for people with chronic disease. This opened our eyes to a serious need in the community, namely, to ensure that treatment and support options are available to everyone across the severity spectrum.

Hunna Watson, PhD, MBiostat, first author
The value of engaged science. I have said this before, but ANGI has been the single most rewarding project I have ever been involved with in my career. The generosity of individuals with anorexia nervosa and their heartfelt desire to “give-back” touched me personally. So many participants willingly gave of their time (and their blood!) in the hope that their contribution would help prevent others from having to endure the suffering that anorexia nervosa had caused for them. I am not sure how best to phrase this, having worked in this field for decades, but there is an inner kernel of humanity that I have seen in every person I have worked with in this field. Too often, I have been able to see it before they can see it in themselves. It is perhaps part of the exquisite interpersonal hypersensitivity that makes them vulnerable to developing the illness in the first place, but when channeled in a healthy direction, it is a gift to the world.
Involving patients, family members, and advocates in engaged science is harder to do than hiding away in the ivory tower, but ultimately imparts more meaning to our work. As stated by our chief statistical analyst Dr. Hunna Watson, “This work was reliant on a worldwide effort of scientists and the community-at-large to bring these novel findings to the fore. The ultimate goal is to capture the causes of anorexia nervosa so that the devastating personal and family toll of this illness can one day be averted.”
