by Emily Carrino
Emily is a rising third year clinical psychology graduate students at UNC and was a CEED summer intern.
People in the United States are increasingly identifying as gay, lesbian, bisexual, or another minority sexual orientation (5.6% of the population; 18.5 million people; Jones, 2021). This growing population generally experiences worse physical, emotional, and relational outcomes than their heterosexual counterparts (e.g., King et al., 2008). Emerging research also suggests that the mental health of those who are bisexual, pansexual, queer, or as another non-monosexual identity, also referred to as “bisexual+” (Davila et al., 2019), experience these difficulties at the highest rates compared to heterosexual people and other subgroups of sexual minorities (Ehlke et al., 2020, Ross et al., 2018). In eating disorder research specifically, gender and sexual orientation, which are distinct constructs, interact to predict prevalence of eating disorders. That is, men who are gay or bisexual experience eating disorders at higher rates than heterosexual men; while the same pattern is not true for women. Lesbian, bisexual, and heterosexual women do not differ in eating disorder prevalence (Feldman & Meyer, 2007). Whereas, the romantic relationships of bisexual+ individuals are understudied, initial findings suggest that these couples may be at higher risk of conflict and other poor outcomes compared to both heterosexual and gay/lesbian couples (Goldberg et al., 2018; Mark et al., 2020). Why?
Gender and Sexuality within Relationships
When sexual minorities form an intimate relationship with another person, each partner has their own gender (male, female, non-binary, etc.) and sexual orientation (who they are romantically or sexually attracted to)—and these are separate phenomena, gender and sexual orientation—which may be the same or different from their partner’s. So, couples might represent a variety of different combinations of sexual orientations and gender. The majority of research about romantic and sexual relationships of sexual minority couples, however, has primarily looked at the gender-makeup of the couple (i.e., the gender combination of each partner), using terms such as “same-sex” and “different-sex” couples to describe their populations; the sexual orientations of the two partners have been neglected. In fact, 100% of couple therapy treatment outcome studies assumed participants’ sexual orientation based upon the gender appearance of their partner (Spengler et al., 2018). Specifically, treatment studies have focused on couples including one male and one female and have assumed that both partners are heterosexual. In rare cases in which sexual orientation was assessed, the options presented to participants were limited to “gay” or “lesbian”; no options were provided for bisexual, pansexual, or other orientations. Therefore, the potential for understanding differences in outcomes based on a bisexual+ orientation within a couple was limited. This is a notable gap in the study of sexual minority couples, and specifically bisexual+ couples of any gender.
This lack of sexual orientation assessment in prior studies also limits our understanding of couples in which the two partners have different sexual orientations (e.g., one female bisexual+ partner and one male heterosexual partner, or one gay male partner and one bisexual+ male partner) versus the SAME orientations. Even less is known about the experiences of mixed-gender (i.e., one man and one woman) sexual minority couples. This unique subset of couples includes one partner who is bisexual+ and one partner who identifies across any spectrum of sexual orientation (heterosexual, bisexual+, or gay/lesbian) and couples in which both partners are bisexual+. Of particular interest within this group is the mix of heterosexual and bisexual+ individuals in relationships. When both the male and female partners in a couple are bisexual+, they are both individual sexual minorities and identify with the sexual minority community, but may seemingly “present as a heterosexual couple” to the outside world based on their visible gender characteristics (i.e., being a man and a woman couple). In couples in which one partner is heterosexual and one partner is bisexual+, there may be additional difficulties experienced as a result of being discordant in their sexual identities. Thus, a prominent and clinically vulnerable subgroup of sexual minority couples, mixed-gender couples with bisexuality+ present, has received little attention in the literature.
This is a striking gap given that when we look at the interaction between sexual orientations of the couple and gender makeup of the couple within bisexual couples, we see that in fact, the vast majority (84%) of partnered bisexual individuals are with a different-gender partner (Pew Research Center, 2015).

Individual and Couple Functioning: Sexual Minority Stress
Extensive research about individual functioning of sexual minorities shows that sexual orientation of individuals, in addition to their gender, is also an important predictor of differential outcomes for sexual minorities, particularly for bisexual+ individuals. That is, in addition to research showing overall worse functioning for sexual minority individuals, bisexual+ individuals seem to be at a particularly high risk of poor outcomes compared to those who are heterosexual, gay, and lesbian. So, broadly speaking, we know that sexual minorities, are not doing well compared to heterosexual individuals. This is based primarily sexual minority stress theory (Meyer, 2003).
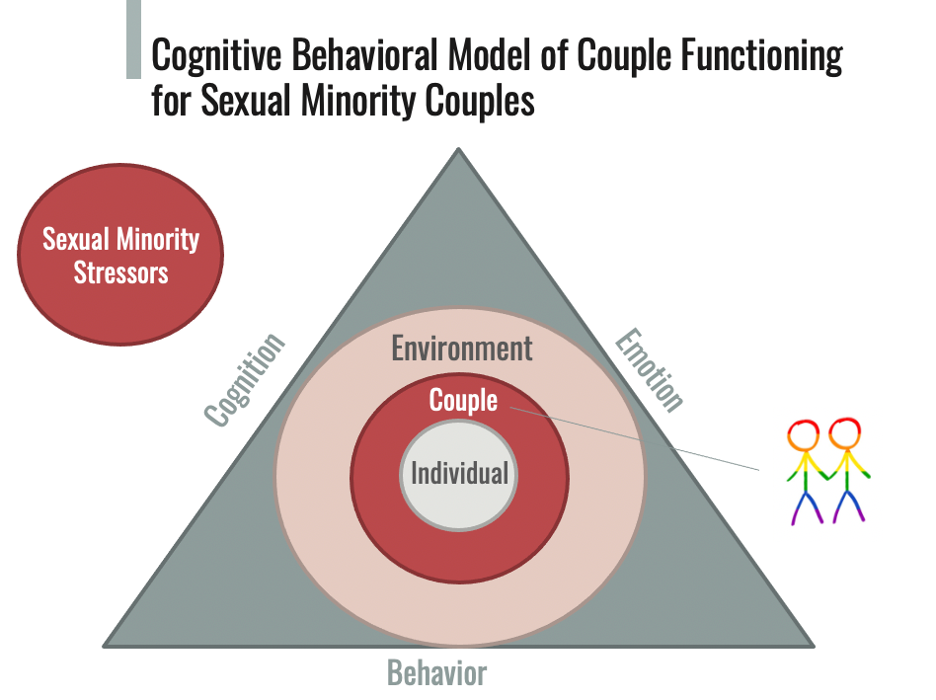
Individuals and couples who have sexual minority orientations may experience a variety of stressors stemming from negative societal attitudes and conditions towards sexual minority individuals and couples. Sexual minorities, people who experience romantic and/or sexual attraction to same-gender or gender-diverse others, experience a wide range of stressors, including discrimination and violence, prejudice, and internalized negative attitudes about themselves. Meyer (2003) gave a name to these collections of experiences: sexual minority stress. There are two main categories of stressors: distal stressors, which are objective events and conditions in one’s environment (for example, prejudice events such as discrimination and violence, or structural inequalities such as limits on same-sex marriage). Proximal stressors, on the other hand, develop through one’s own perceptions and appraisals of distal stressors, leading to psychological impacts that are internalized by the individual or couple. These proximal, psychological stressors include expectations of rejection, concealment of identity, and internalized homonegativity. Experiences of sexual minority stress may influence a couple’s well-being by way of three domains from an ecological perspective: (a) the individuals who make up the relationship, (b) how the two partners interact as a couple, and (c) their environment and how the couple exists in a broader community (Baucom et al., 2020). Risk and protective factors that determine the qualities of one’s relationship exist on all three levels. At the individual level, what each partner brings into the relationship (e.g., mental health concerns, specific sexual orientation) might influence the other partner’s well-being and the couple’s well-being in a variety of ways. At the couple level, different interaction patterns and relational qualities between the two partners (e.g., communication quality, level of intimacy, conflict as a result of discrepant sexual orientations) and their effects on the couple can be examined. Further, individual and relationship functioning are inextricably tied such that they influence one another (Baucom et al., 2020).
Moreover, each partner’s own well-being and daily stressful experiences can influence the other partner’s well-being and overall stress (e.g., Peterson et al., 2008). Thus, individual and relational factors, both risk and protective, contribute to the overall functioning of individuals and their romantic relationship. For example, the presence of an eating disorder within a couple may cause disruptions to the couple’s daily routines, sense of closeness and intimacy, conflict, etc. (Bulik et al., 2011). Additionally, facets of the couple’s environment can impact individual and couple functioning (Baucom et al., 2020). These environmental factors can include positives that benefit the couple (e.g., social support from friends or family) and/or negatives that have the potential to harm the couple (e.g., experiences of discrimination based on sexual identity, laws that discriminate against same-gender couples).
Given that not all sexual minorities experience the same sexual minority stressors, or the same minority stressors in the same way, it is important to consider what factors might drive differences in experiences of sexual minority stress, and ultimately, overall individual and relationship functioning, of between heterogeneous groups of sexual minority couples.
As a starting point, scholars and clinicians can ask themselves:
- How have I assessed for and understood sexual orientation in my research populations and patients? What groups and subgroups would I like to include in future work?
- What role might gender and sexual orientation have in my specific area of focus (for example, binge-eating spectrum disorders)? Why?
- How can I better cater to the needs of sexual minority (and specifically, bisexual+) individuals and couples in my research and clinical work?
By asking these questions, researchers can ensure that they are not making assumptions about the individuals they are studying based just on observable characteristics and acknowledge and embrace the complexity of human interpersonal relationships.
References
Baucom, D. H., Fischer, M. S., Corrie, S., Worrell, M., Boeding, S. E. (2020). Treating relationship distress and psychopathology in couples. Routledge. New York, NY.
Bulik, C. M., Baucom, D. H., Kirby, J. S., & Pisetsky, E. (2011). Uniting couples (in the treatment of) anorexia nervosa (UCAN). The International Journal of Eating Disorders, 44(1), 19-28. https://doi.org/10.1002/eat.20790
Davila, J., Jabbour, J., Jabbour, J., Dyar, C., Dyar, C., Feinstein, B. A., & Feinstein, B. A. (2019). Bi+ visibility: Characteristics of those who attempt to make their bisexual+ identity visible and the strategies they use. Archives of Sexual Behavior, 48(1), 199-211. https://doi.org/10.1007/s10508-018-1284-6
Ehlke, S. J., Braitman, A. L., Dawson, C. A., Heron, K. E., & Lewis, R. J. (2020). Sexual minority stress and social support explain the association between sexual identity with physical and mental health problems among young lesbian and bisexual women. Sex Roles, 83(5-6), 370-381. https://doi.org/10.1007/s11199-019-01117-w
Feldman, M. B., & Meyer, I. H. (2007). Eating disorders in diverse lesbian, gay, and bisexual populations. The International Journal of Eating Disorders, 40(3), 218-226. https://doi.org/10.1002/eat.20360
Goldberg, A., Garcia, R., & Manley, M. (2018). Monosexual and nonmonosexual women in same-sex couples’ relationship quality during the first five years of parenthood. Sexual and Relationship Therapy, 33(1-2), 190-212. https://doi.org/10.1080/14681994.2017.1419561
Jones, J. (February 24, 2021). LGBT Identification Rises to 5.6% in Latest US Estimate. Gallup.
King, M., Semlyen, J., Tai, S. S., Killaspy, H., Osborn, D., Popelyuk, D., & Nazareth, I. (2008). A systematic review of mental disorder, suicide, and deliberate self harm in lesbian, gay and bisexual people. BMC Psychiatry, 8, 70. http://dx.doi.org/10.1186/1471-244X-8-70
Mark, K. P., Vowels, L. M., Bunting, A. M. (2020). The impact of bisexual identity on sexual and relationship satisfaction of mixed sex couples. Journal of Bisexuality, 20(2), 119-140. https://doi.org/10.1080/15299716.2020.1734137
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674-697. https://doi.org/10.1037/0033-2909.129.5.674
Peterson, B. D., Pirritano, M., Christensen, U., & Schmidt, L. (2008). The impact of partner coping in couples experiencing infertility. Human Reproduction, 23, 1128–1137. https://doi.org/10.1093/humrep/den067
Pew Research Center. (2015). Among LGBT Americans, bisexuals stand out when it comes to identity, acceptance. Retrieved January 3, 2021 from https://www.pewresearch.org/fact-tank/2015/02/20/among-lgbt-americans-bisexuals-stand-out-when-it-comes-to-identity-acceptance/
Ross, L. E., Salway, T., Tarasoff, L. A., MacKay, J. M., Hawkins, B. W., & Fehr, C. P. (2018). Prevalence of depression and anxiety among bisexual people compared to gay, lesbian, and heterosexual individuals: A systematic review and meta-analysis. The Journal of Sex Research, 55(4-5), 435-456. https://doi.org/10.1080/00224499.2017.1387755
Spengler, E. S., DeVore, E. N., Spengler, P. M., & Lee, N. A. (2020). What does “Couple” mean in couple therapy outcome research? A systematic review of the implicit and explicit, inclusion and exclusion of gender and sexual minority individuals and identities. Journal of Marital and Family Therapy, 46(2), 240-255. https://doi.org/10.1111/jmft.12415
